Magnesium is the fourth most abundant cation in the human body and the second most prevalent intracellular cation after potassium. It plays a central role in human physiology, acting as an essential cofactor in more than 300 enzymatic reactions that regulate energy metabolism, glucose homeostasis, protein synthesis, nucleic acid stability, and neuromuscular function. Despite its fundamental biological importance, magnesium deficiency remains underrecognized in clinical practice and public health, particularly in populations with metabolic disorders.

Recent decades have witnessed a growing body of scientific evidence linking suboptimal magnesium status to insulin resistance, metabolic syndrome, type 2 diabetes mellitus, cardiovascular disease, and chronic low-grade inflammation. These associations have driven renewed clinical interest in magnesium not only as a micronutrient but also as a therapeutic adjunct in metabolic and endocrine disorders.
Clinical Summary of Magnesium
Magnesium is involved in virtually every major metabolic pathway in the body. Approximately 50-60% of total body magnesium is stored in bone, while the remainder resides in muscle and soft tissues, with less than 1% present in extracellular fluids. This distribution underscores why serum magnesium levels often fail to reflect total body magnesium status.
Clinical research has consistently demonstrated that magnesium plays a regulatory role in glucose transport, insulin signaling, lipid metabolism, mitochondrial function, and inflammatory modulation. According to the study published in American Journal of Clinical Nutrition by Rude described that magnesium deficiency disrupts cellular energy metabolism and increases susceptibility to metabolic and cardiovascular diseases.
From a clinical perspective, magnesium insufficiency has been associated with fatigue, muscle cramps, neuromuscular irritability, impaired glucose tolerance, and increased cardiometabolic risk. Importantly, magnesium repletion has been shown to improve metabolic markers in both deficient and at-risk individuals.

Magnesium Deficiency: Prevalence and Clinical Implications
Magnesium deficiency, often referred to as hypomagnesemia when severe, is increasingly prevalent due to modern dietary patterns, food processing, soil mineral depletion, and lifestyle factors. Epidemiological studies suggest that a significant proportion of adults fail to meet recommended magnesium intake levels.
Elin highlighted in the journal of Clinical Chemistry that chronic marginal magnesium deficiency may remain clinically silent for years while progressively contributing to metabolic dysfunction and type 2 diabetes. Deficiency impairs insulin receptor activity, promotes oxidative stress, enhances inflammatory cytokine production, and alters calcium and potassium homeostasis. These disturbances create a biochemical environment conducive to metabolic syndrome and glucose dysregulation.
Magnesium Consumption and Regulation in the Body
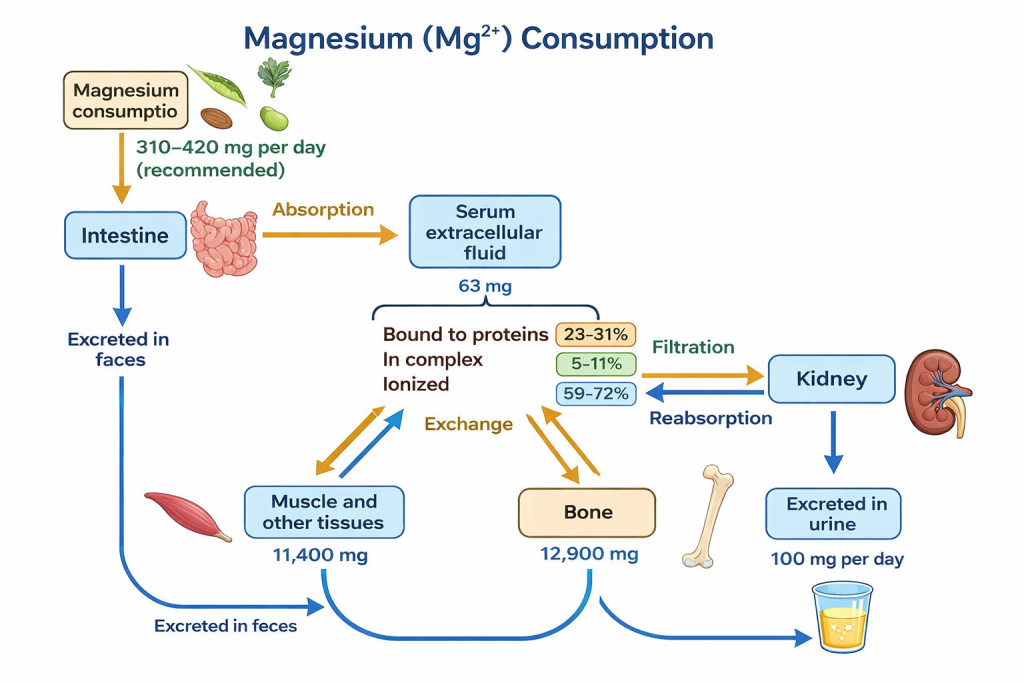
According to comprehensive study published in the journal of Health Sciences Review by Luis Soriano-Pérez et al, described that Magnesium (Mg²⁺) is an essential mineral that the body needs every day to function properly. Adult men require about 420 mg per day, while adult women need around 320 mg, and most of this magnesium comes from food. Good dietary sources include leafy green vegetables such as spinach, legumes (peas and beans), nuts, seeds, and whole-grain cereals. In total, the adult human body contains about 24 g of magnesium, most of which is stored in bones, with the rest found in muscles and other soft tissues. The balance of magnesium in the body is carefully controlled by the intestine, bones, and kidneys.
Typical overview of Magnesium homeostasis in the body is maintained through intestinal absorption, circulation as ionized and protein-bound forms, dynamic exchange with bone and tissues, and precise regulation via renal filtration, reabsorption, and urinary excretion. NOTE: The dose of Magnesium as per FSSAI is 440mg (Adult Men) and 370mg (Adult Women).
When magnesium is consumed in the diet, only about 30-50% is absorbed in the intestines; the remaining amount is eliminated in the stool. Most absorption takes place in the small intestine through a passive process that depends on magnesium concentration, accounting for nearly 90% of total uptake. A smaller but important portion is absorbed in the large intestine through specialized channels called TRPM6 and TRPM7, which help move magnesium into intestinal cells, especially when intake is low.
After absorption, magnesium enters the bloodstream, where its level reflects how much is consumed in the diet. With recommended intake levels, about 63 mg of magnesium circulates in the blood. Bones act as the main storage site and can release magnesium when the body needs it. The kidneys play a key role in preventing magnesium loss by reabsorbing most of the filtered mineral before it is excreted in urine.
Magnesium deficiency can occur due to poor dietary intake, reduced absorption, increased urinary loss, or inherited conditions. Low blood magnesium levels (hypomagnesemia) are common in many populations, particularly in Western-style diets that provide only 30-50% of the recommended daily magnesium intake.
Hormonal factors, including insulin, parathyroid hormone, and vitamin D, influence magnesium distribution and retention. Notably, insulin resistance itself impairs cellular magnesium uptake, creating a vicious cycle in which magnesium deficiency exacerbates metabolic dysfunction, further worsening magnesium status.
Physiological and Metabolic Functions of Magnesium
Central Role in Metabolic Regulation
Barbagallo and Dominguez, writing in Current Opinion in Clinical Nutrition and Metabolic Care, demonstrated Magnesium is a vital micronutrient that serves as a cofactor for over 300 enzymatic reactions, playing a central role in energy metabolism. It stabilizes ATP as a magnesium-ATP complex (This complex is essential for nearly all ATP-dependent biochemical reactions, including those involved in carbohydrate, lipid, and protein metabolism), enabling nearly all ATP-dependent biochemical processes. Magnesium supports key enzymes involved in glycolysis, the tricarboxylic acid cycle, and oxidative phosphorylation, thereby regulating glucose utilization and mitochondrial energy production. It also directly modulates insulin signaling by facilitating insulin receptor autophosphorylation and downstream pathways essential for glucose uptake. Additionally, magnesium influences lipid metabolism and protein synthesis, positioning it as a key regulator of metabolic efficiency and cellular energy homeostasis.
Magnesium and Metabolic Syndrome
Metabolic syndrome represents a complex clustering of interrelated metabolic abnormalities, including central obesity, insulin resistance, dyslipidemia, hypertension, and chronic low-grade inflammation. A consistent finding across epidemiological, clinical, and mechanistic studies is the high prevalence of magnesium deficiency among individuals with metabolic syndrome, suggesting that magnesium insufficiency functions both as a contributing factor and as a metabolic consequence of the syndrome.
Guerrero-Romero, in the journal of Diabetes & Metabolism, provided early mechanistic evidence that low intracellular magnesium concentrations impair insulin receptor tyrosine kinase activity. This impairment disrupts insulin signal transduction, leading to reduced phosphorylation of insulin receptor substrates and attenuation of downstream PI3K-Akt signaling. As a result, glucose transporter type 4 (GLUT4) translocation to the cell membrane is diminished, limiting glucose uptake in skeletal muscle and adipose tissue and promoting systemic insulin resistance.
This insulin resistance initiates a cascade of metabolic disturbances. Reduced glucose disposal leads to chronic hyperglycemia, which stimulates compensatory hyperinsulinemia. Elevated insulin levels, in turn, favor adipocyte hypertrophy, particularly in visceral fat depots, thereby exacerbating central obesity. Magnesium deficiency further compounds these effects by impairing mitochondrial ATP generation, reducing metabolic flexibility, and increasing oxidative stress, all of which are hallmarks of metabolic syndrome.
Magnesium also plays a crucial role in modulating inflammatory pathways that underlie metabolic syndrome. Adequate magnesium status inhibits the activation of nuclear factor-κB (NF-κB), a transcription factor that regulates the expression of numerous pro-inflammatory cytokines. Magnesium deficiency has been shown to promote NF-κB activation, leading to increased production of tumor necrosis factor-α (TNF-α), interleukin-6 (IL-6), and C-reactive protein. These inflammatory mediators interfere with insulin signaling, promote endothelial dysfunction, and contribute to the chronic inflammatory state characteristic of metabolic syndrome.
In the vascular system, magnesium deficiency increases intracellular calcium concentrations within vascular smooth muscle cells, promoting vasoconstriction and elevating peripheral resistance. This mechanism provides a physiological explanation for the strong association between low magnesium status and hypertension observed in individuals with metabolic syndrome.
Thus, magnesium deficiency contributes simultaneously to insulin resistance, inflammation, dyslipidemia, and hypertension, reinforcing the multifactorial nature of the syndrome.
Magnesium and Type 2 Diabetes Mellitus
The relationship between magnesium and type 2 diabetes mellitus (T2DM) is one of the most extensively investigated areas in micronutrient research. A substantial body of evidence from prospective cohort studies, randomized controlled trials, and meta-analyses consistently demonstrates an inverse association between magnesium intake and the risk of developing type 2 diabetes.
Larsson and Wolk, in the Journal of Internal Medicine, reported that individuals with higher dietary magnesium intake exhibited a significantly lower incidence of type 2 diabetes. This protective association remained robust after adjustment for body mass index, physical activity, and other dietary factors, indicating an independent role of magnesium in glucose homeostasis. Mechanistically, magnesium enhances insulin sensitivity by facilitating insulin receptor function, improving downstream signaling efficiency, and supporting GLUT4 translocation to the cell membrane.
At the cellular level, magnesium stabilizes phospholipid membranes and modulates ion transport, thereby maintaining optimal cellular responsiveness to insulin. In pancreatic β-cells, magnesium contributes to glucose-stimulated insulin secretion by regulating ATP-dependent potassium channels and calcium influx, both of which are essential for insulin exocytosis. Magnesium deficiency disrupts these processes, leading to impaired insulin secretion and further deterioration of glycemic control.
Clinical intervention studies have provided additional support for magnesium’s therapeutic relevance in type 2 diabetes. Supplementation trials have demonstrated improvements in fasting plasma glucose, glycated hemoglobin (HbA1c), and insulin sensitivity indices, particularly in individuals with documented hypomagnesemia. These benefits are attributed to restored intracellular magnesium levels, improved insulin receptor activity, reduced oxidative stress, and attenuation of chronic inflammation.
Importantly, type 2 diabetes itself promotes magnesium depletion through increased urinary magnesium excretion driven by hyperglycemia-induced osmotic diuresis. This creates a self-perpetuating cycle in which magnesium deficiency worsens insulin resistance and glycemic control, which in turn accelerates further magnesium loss.
Breaking this cycle through adequate dietary intake or targeted supplementation has therefore emerged as a clinically relevant strategy in diabetes management.
Key Takeaway: Collectively, current evidence positions magnesium as a foundational micronutrient in metabolic health. Its roles in energy metabolism, insulin signaling, inflammatory regulation, and vascular function explain why magnesium deficiency is so closely linked to metabolic syndrome and type 2 diabetes. Maintaining adequate magnesium status is not only essential for metabolic homeostasis but also represents a practical and evidence-based approach to reducing cardiometabolic risk.
Magnesium Supplements: Forms and Applications
When dietary intake is insufficient or physiological demand is elevated, magnesium supplementation becomes clinically relevant. Supplemental magnesium is available in inorganic and organic salt forms, each differing in bioavailability and gastrointestinal tolerance.
Organic forms such as magnesium citrate, glycinate, malate, and lactate generally exhibit superior absorption compared to inorganic forms like magnesium oxide. A study published in the Journal of the American College of Nutrition, demonstrated that magnesium citrate resulted in significantly higher bioavailability than magnesium oxide.
The choice of supplement should align with clinical goals, tolerance, and regulatory compliance within nutraceutical formulations.
What to Consider Before Choosing the Right Magnesium Supplement
Selecting an appropriate magnesium supplement requires consideration of bioavailability, elemental magnesium content, gastrointestinal tolerance, target population, and intended clinical outcome. Factors such as dosage form, combination with other micronutrients, and timing of administration influence efficacy.
From an industry standpoint, regulatory frameworks such as FSSAI, EFSA, and US FDA guidelines govern permissible forms and dosage limits, which must be considered during product development.
Clinical Uses of Magnesium
Clinically, magnesium is used in the management of hypomagnesemia, metabolic syndrome, type 2 diabetes, hypertension, migraine, premenstrual syndrome, and neuromuscular disorders. In hospital settings, intravenous magnesium is used for preeclampsia, torsades de pointes, and acute asthma exacerbations.
In nutraceutical practice, magnesium is increasingly incorporated into formulations targeting metabolic health, stress modulation, sleep quality, and musculoskeletal function.
Dose Recommendations
Recommended dietary allowances (RDA) for magnesium vary by age, sex, and physiological status. Adult men typically require higher intake than women, while pregnancy and lactation increase magnesium requirements.
Clinical supplementation doses generally range from 200-400 mg elemental magnesium per day, depending on indication and baseline status. Therapeutic dosing should align with regulatory guidelines and individual tolerability.
Bottom Line
Magnesium is a cornerstone micronutrient in human metabolism with profound implications for metabolic health, insulin sensitivity, and chronic disease prevention. Subclinical deficiency is widespread and contributes silently to the burden of metabolic syndrome and type 2 diabetes.
Scientific evidence strongly supports the role of adequate magnesium intake through diet and supplementation as a safe, effective, and evidence-based strategy for improving metabolic outcomes. For clinicians, researchers, and nutraceutical professionals, magnesium represents both a fundamental nutritional requirement and a clinically relevant therapeutic tool.
Disclaimer: This article is for educational purposes only and does not substitute professional medical advice. Pregnant women should consult qualified healthcare providers for dietary guidance.
Read Articles Below for More Health Update
Magnesium Deficiency and Aging: Impact on Cells, Skin Health, and Longevity
Liver Disease: Epidemiology, Pathophysiology, Stages of Damage, Causes, Symptoms, and Management
High Protein Intake and Kidney Damage: What Research Really Says